
BY DR. BAYNE FRENCH, MD DC
I have some unfortunate news for you. You’re part of a population. In college I wanted to major in Populus Avoidance. My guidance counselor didn’t give me any guidance. In fact, she didn’t even want to meet with me. I was used to that. She claimed that academic major didn’t even exist. I eventually gave up and decided on pre-med.
There’s a lot of problems with the populus. Pestilence, crime, chit chat, and others. Also, as a member, you are subject to medical advice from population-based studies. You know, looking at the masses. But you’re not a population, you’re an individual. One with your own unique collection of risk factors, and genetic baggage.
Population-based recommendations are efficient. They’re simple, quick, and have the advantage of being “evidence-based”. Individualized medical recommendations are far more nebulous, time consuming and require more dialogue…things most medical providers intend to avoid. The system is not set up to allow for this on a large scale. There are powerful forces at work, under the guise of value-based care, that require us (me) to fill out forms. Heaps of them. Useless forms, that cannot be delegated to others. My view of “value” is me in the room with a patient. Every year it gets harder to do that. Behind these abysmal decisions and mandates are people. Idiots. I would love to get in the octagon with a few of them. Not that I know what I’m doing in there but they’d be missing an ear when I was through.
Plugging you, a gnarly, aggressive, and gorgeous zebra into guidelines designed for a horse is not a style of medical practice that I overly enjoy. I want to have individualized discussions with individual patients. I want them to read and research and ask questions. I am unfazed, completely unaffected when patients choose to not take my advice. It does not offend me. I don’t have time to be offended because in order to practice the way I want, there is a heightened level of efficiency that needs to take place. This usually starts at 5 AM when I go through every patient on my schedule. It also involves an intolerance of patients being late. No-shows result in a search for a new doctor. I can operate this way because I work at an independent clinic, a zebra in its own right not subject to decisions and mandates of a conglomerate. For most providers in the United States this scenario is an impossibility. As it is for most dedicated providers in my region.
Maybe you can now understand why your Stiff in a White Coat wants to put you on Lipitor when your cholesterol is high. Not because they’re bad people. It’s a bad, broken, sick-focused system. If you don’t want to be a part of it then listen the hell up!
Action Items:
If you have a clogged toilet, you don’t call a mechanic, right? First turn on the ceiling fan. If you have a broken bone, you probably shouldn’t see a chakra reader for it. If you want a Western Medicine method of treating disease, then most medical providers will suffice. Not if you want to understand health, wellness and true prevention (I don’t mean “early detection”). You’re largely on your own for that. You must be curious, and motivated to be well. You must be willing to look hard at your own dogma, upbringing, relationship with food, habits, and your incessant excuse making. As one of my idols Dr. Bernie Roth said “reasons are prettied up excuses”. You must be willing to READ. This quest may also benefit from consultations with Naturopathic physicians, or Functional Medicine trained providers. If the first question out of your mouth is “does insurance cover that?”, then just take the damn Lipitor.
With every article I write, there results some comments and questions. A common theme is a desire for “ammunition” to convince their respective provider why they don’t need to take cholesterol medicine. My first advice is to stop trying to convince anyone of anything. Our human demise would be delayed if we all just stopped trying to do that. Especially when dealing with indoctrinated “experts” like physicians. Stop it. Instead educate yourselves. What you might find is that taking cholesterol medicine is the right move. Especially if you’ve developed a belly, your father died relatively young, you’ve developed Fatty Liver Disease, and you’re not willing to stop eating carb as a staple. And especially if you smoke.
What are statins anyway?
Because I’m lazy, I’m just going to include narrative I wrote from a previous article:
The statins are a group of medications that interfere with cholesterol production. They have been widely purported to lower the risk of cardiovascular disease and heart attacks. There are few things within medicine that are so vehemently clung to as this concept. The status quo is powerful here and although massive amounts of data over decades have brought into question the rationale for widespread use of these drugs, most medical providers do not deviate from their fervent dogma.
Nilsson et al. (J Negat Results Biomed. 2011) performed a very large study looking at individuals between 1998 and 2002 in regards to statin use and heart attacks and death. “Though a widespread and increasing utilization of statins, no correlation to the incidence or mortality of AMI (heart attack) could be detected”.
There is certainly something powerful biologically going on with statin medications. In addition to lowering cholesterol, they lower inflammation, and act as antioxidants. To say that they are universally beneficial and indicated for everyone with elevated cholesterol is grossly inaccurate. Like Kenny Rogers said, “You’ve got to know when to hold ‘em, know when to fold ‘em”. Statins likely help reduced cardiovascular disease in certain situations. Like men under 70 who have already had a heart attack, and men with numerous risk factors (elevated blood pressure, abdominal obesity, diabetes, smoking, etc). As Abramson et al (BMJ. 2013) reported, for the majority of people for which statins are prescribed (specifically for “primary prevention”, people who DO NOT have heart disease) the benefit is lacking, while side effects and risks are significant.
Very often the “36% reduction” in heart attacks attributable to statin treatment is mentioned with little understanding of what that actually means. It is a statistical figure referring to relative risk reduction. The actual reduction in heart attacks was 1% (3% down to 2%). This is absolute risk reduction. The benefit of statin medication for relatively healthy people, without known heart disease, is just not there. A group of independent researchers reviewed vast data (Cochrane Database Systematic Reviews) found the evidence limited that statins help prevent a first heart attack, and “caution” should be taken in prescribing them for this reason (75% of statin prescriptions are written for low-risk patients).
An independent (no industry funding) group of doctors and scientists formed a group whose foundation is a concept called NNT (number needed to treat). It is a way of looking at the real benefit and risk of a treatment. Their work on statins (and other interventions) can be found at www.thennt.com. It is not favorable in regards to statin use.
Dr. Bernie Roth said: “Experimental verification is itself also a rather imperfect tool. I think it is important to understand that every time someone uses science or research, he is not talking about the work of some omnipotent beings with access to revealed truths but of fallible people working in a currently accepted paradigm and socialized into a scientific family and job structure.” Bernie knows that well intentioned “experts” make mistakes all the time. And that initially well-intentioned researchers can easily be swayed by funding, grants, and promise of career advancement.
Metabolism Defined:
This is very important for you to understanding, as most disease (stroke, heart attack, Alzheimer’s, diabetes, obesity, cancers) are different versions of abnormal metabolism over time.
Metabolism defined, from a previous article: “Dr. Vanderkooi in Your Inner Engine: An Introductory Course on Human Metabolism defines cellular metabolism as “the process by which the products of digestion are chemically modified to yield usable energy.” You eat stuff, it gets broken down in the digestive tract, and those tiny food bits get absorbed across the intestinal lining into the bloodstream, and then “metabolized.” Many diseases including cardiovascular, type 2 diabetes (T2D) and cancers occur when normal metabolism is disrupted.”
YOUR Data:
- Cholesterol. This is what we’re talking about right? “Ammunition” for you to avoid statin medication. In Lipids. A Different Perspective I wrote way, way too much about cholesterol. It’s a sticky-wicket, a slippery-slope, and other cliches I can’t think of right now. Stop pressuring me. There are advanced cholesterol panels that can be ordered. The ordering is the easy part, but who’s going to interpret the results? If you have a provider who actually understands the NMR panel, then sing zippity doo dah. If not then just look at the old, boring, original cholesterol panel. Particularly the Triglyceride value OVER the HDL value. Yep, fat over good cholesterol. I view it as the most powerful independent predictor of who gets a heart attack. There’s a tipping point of about 2.8-3 (an example of a ratio of 3 is triglyceride of 150 and HDL of 50). This value and higher results in a significantly elevated risk of heart attacks, and is a sign of being metabolically unwell.
- Liver Function Tests, AKA LFT’s. I’ve written about all the versions of a fatty liver that can and likely will befall those carb-addicted among you. Carb is converted to fat. Some make this conversion very well, others less efficiently, but we all do it well thanks to our fore-people and survival of the best-fat-makers. This fat is stored EVERYWHERE, including in the liver. Fois Gras anyone?
Liver function tests are routine, and a part of the CMP (Comprehensive Metabolic Panel), a test you’ve all had. If your ALT and AST are in the 20’s I bow before you. 30’s I won’t bow. 40’s and the chance of NAFLD (Nonalcoholic Fatty Liver Disease) is relatively high. This means you’re metabolically unwell. The chance of statin medication like Lipitor helping you just went up. - Uric Acid. This will be a separate tome so I’ll be brief. Many consider this the “gout test”, but it’s so much more. It is a metabolic disease driver, and its connection with cardiovascular disease was first recognized in 1879. Like most things metabolic, we each have a unique genetic predisposition but what is clear is that sugar is a potent contributor to uric acid formation. An ideal uric acid level is less than 5.
- Iron. I wrote about this in “Laboratory Testing-New Things to Consider”. And more recently in a blood donation article. There are many biochemical mechanisms whereby increased total body iron can contribute to cardiovascular disease. The iron measurement usually done is ferritin. Even a modest elevation of ferritin of around 200 has a 2.2-fold increase in heart attacks. As if our government-recommended high cereal consumption isn’t bad enough, let’s iron fortify them! Idiots.
Have your ferritin checked, along with a CRP which measures inflammation. If your CRP is normal, the ferritin level is likely accurate. An optimal level is around 70. If it’s high, that iron can oxidize your cholesterol, making it particularly bad, making Lipitor a bit more prudent. Or just read my last blood donation article. Jeez. - Homocysteine. This is an intermediary non-protein amino acid. Interestingly this compound can drive numerous pathways leading to cardiovascular disease. You should know your homocysteine levels. Certain B vitamins can lower, or at least neutralize homocysteine.
- C-Reactive Protein. This is a normal chemical in our body and is a nonspecific marker of inflammation. Numerous studies have shown predictive value in CRP measurements as a predictor of cardiovascular disease. If you are not obviously sick or injured, and your CRP is elevated it at least needs to be repeated in a few weeks. The COVID vaccine and boosters can result in rather dramatic elevations of this test. If it remains elevated I view this as a metabolic problem, and your shitty cholesterol just became a bigger deal.
- Hemoglobin A1c. This is a measure of how sugar sticks to protein, all protein, but specifically to the protein in our red blood cells called hemoglobin. What once was only viewed as a test useful to determine the blood sugar control of patients with diabetics, and A1c is a revealing measure of metabolic health. I like 5.5 or less. Over that and glycation (sugar sticking) is taking place at an accelerated rate and your crappy cholesterol just became a much bigger deal.
- Omega-3 Index. This is a test you order on your own and is usually less than $100. It measures how much heart healthy Omega-3 fats you have in your body. I’ve written extensively about this too and the importance of minimizing the Omega 6 fats while increasing the Omega-3’s. You want to have a high index, over 8%. Less than 4% and maybe Lipitor may actually help you remain undead.
- Cortisol. I’ve written an article on cortisol. It is a stress hormone that has numerous and varied functions, including on our metabolism. Since most of us will die of metabolic disease, evaluating your “cortisol curve” might guide healthful changes. The cortisol curve is the rhythm of cortisol release during the day and is best determined using four-point saliva testing. These test kits are widely available, and like the Omega-3 Index test, you can do this testing on your own.
Cortisol abnormalities, particularly excess, elevates blood pressure, cravings, appetite, and abdominal girth. Collectively, heart disease risk increases. - Abdominal girth. Increasing weight, and body mass index (BMI) correlate with an increased risk of heart disease. It appears that a better predictor of heart risk is by waist size. Where excess fat is stored is important, and belly fat is the worst. There are several large studies that look at this and have established not just a correlation, but causality between a larger waist circumference and heart attacks. According to the National Heart, Lung, and Blood Institute, women with waist/abdominal circumference greater than 35 inches and men greater than 40 inches have a much higher risk for both Type 2 diabetes and heart disease.
If you are a regular consumer of carbohydrate, there isn’t a prayer of leaning out in the midsection. Reducing all carb, especially sugar, and intermittent fasting is the best way to burn this abdominal fat, and reduce risk. - Family history of heart disease. What befalls your first degree relatives modifies your own risk, depending on the number and age of affected relatives. Early heart disease is generally considered to be <55 in men and <65 in women. Siblings of individuals with early heart disease have a 40% increased risk. Offspring of those with early heart disease have a 60-75% elevated risk. This obviously represents a non-modifiable risk factor but can be factored in to your overall gestalt of individual risk.
- Sleep. There exists a U-shaped relationship between sleep duration and dying from numerous things including heart disease, cancers, and stroke. The lowest risk is for individuals consistently getting 7-8 hours. If less than 6 or over 9 the risk of dying goes up considerably.
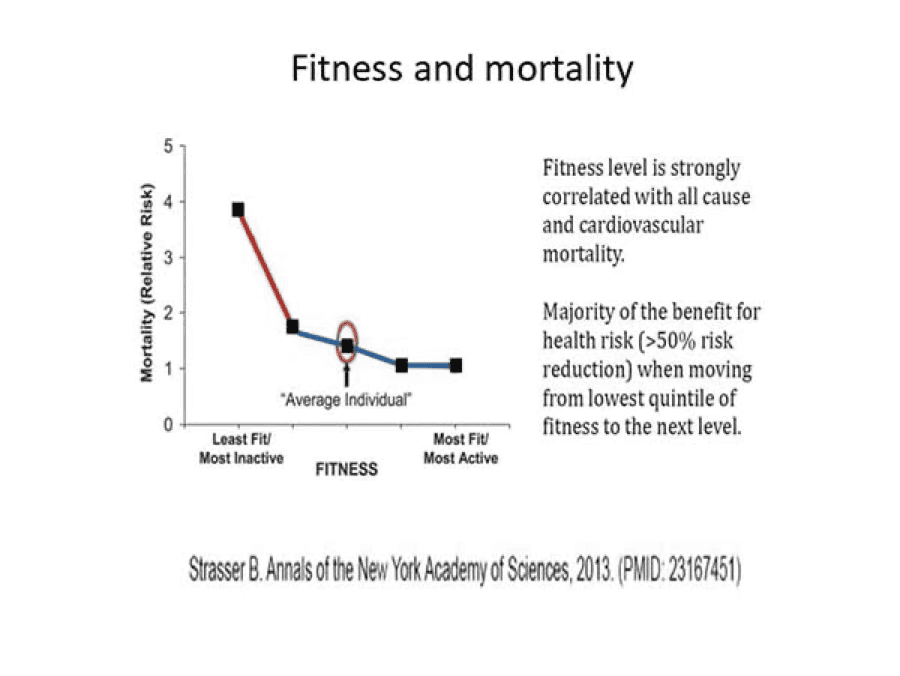
Proper sleep must be prioritized as a way to reduce the risk of metabolic disease. There are several safe medications available. Your medical provider can assist with this, and screen for sleep apnea. - Fitness. This may come as a shock to most of you, but exercise is healthy. The risk of dying is significantly reduced with even a small amount of exercise (as shown in the graph below), and the benefit seems to peak at about 50-60 minutes per day of moderate to vigorous exercise. Medical groups commonly recommend 150 minutes per week of moderate intensity (a level where you can talk but not sing) exercise.
- Hypertension. This is elevated blood pressure.
The American Heart Association and American College of Cardiology divides blood pressure into four categories:
- Normal blood pressure. Blood pressure is 120/80 mm Hg or lower.
- Elevated blood pressure. The top number ranges from 120 to 129 mm Hg and the bottom number is below, not above, 80 mm Hg.
- Stage 1 hypertension. The top number ranges from 130 to 139 mm Hg or the bottom number is between 80 and 89 mm Hg.
- Stage 2 hypertension. The top number is 140 mm Hg or higher or the bottom number is 90 mm Hg or higher.
There is a continuous relationship between elevated blood pressure and heart disease risk. Optimizing blood pressure using medication is in general very effective and traditionally trained medical providers are very good at this. Numerous lifestyle interventions are also helpful, especially reducing abdominal girth and exercising regularily.
Conclusion:
We’re all here for a blink in time. Making the most of it in terms of joy and meaning is very high on my priority list. It’s right up there with getting my 9-year-old to school on time. Having good health and avoiding disease one of the most powerful contributors to a life well lived.
To help ascertain your individual risk, the above factors, metrics, and values should be determined. I feel that with abnormal cholesterol, the more abnormalities you have to the factors above, the potential benefit of statin medication goes up. This is not cookie cutter. It’s not a recipe. It’s individual risk assessment and empowerment through knowledge.
Advocate for yourselves. No one is capable of doing a better job.
← Back to Articles-

Email
Our team is dedicated to providing personalized care and guidance tailored to your individual needs.
Email Us -

Phone
Take the first step towards a healthier you today!
(406) 405-1457 -

Office
We look forward to seeing you.
Whitefish Medical
144A 2nd St
Whitefish, MT 59937